Introduction: The Shift from Reactive to Predictive Healthcare
Healthcare has historically operated on a reactive model—patients seek care after symptoms appear, conditions worsen, or emergencies occur. This approach strains resources, escalates costs, and often leads to suboptimal patient outcomes. The industry is now experiencing a fundamental transformation toward predictive healthcare, where data-driven insights anticipate patient needs before critical events occur.
Predictive patient care leverages artificial intelligence to analyze historical health data, identify patterns invisible to human observation, and forecast future health trajectories. This paradigm shift enables care teams to intervene earlier, personalize treatment plans, allocate resources efficiently, and ultimately save lives while reducing healthcare expenditures.
Salesforce Health Cloud, integrated with Einstein AI, represents one of the most comprehensive platforms for implementing predictive patient care at scale. Unlike generic CRM systems adapted for healthcare, Health Cloud was purpose-built for the complexities of patient relationships, care coordination, and regulatory compliance. When augmented with Einstein’s AI capabilities, it transforms from a record-keeping system into an intelligent care orchestration platform.
This comprehensive guide explores how healthcare organizations can practically implement AI in Salesforce Health Cloud, moving beyond theoretical possibilities to actionable workflows that deliver measurable patient and business outcomes.
Understanding Einstein AI Within Salesforce Health Cloud
What Makes Einstein AI Different in Healthcare Context
Einstein AI isn’t a standalone product but rather an integrated intelligence layer woven throughout the Salesforce ecosystem. In Health Cloud specifically, Einstein adapts its capabilities to healthcare’s unique requirements—HIPAA compliance, longitudinal patient records, multi-provider care coordination, and the criticality of accuracy in clinical contexts.
The distinction is crucial: while consumer-focused AI might tolerate a 5% error rate, healthcare AI must operate with clinical-grade precision while remaining explainable to care teams who bear ultimate accountability for patient decisions. Einstein achieves this through supervised learning models that healthcare organizations can train on their own patient populations, creating algorithms that reflect their specific patient demographics, regional health challenges, and care delivery models.
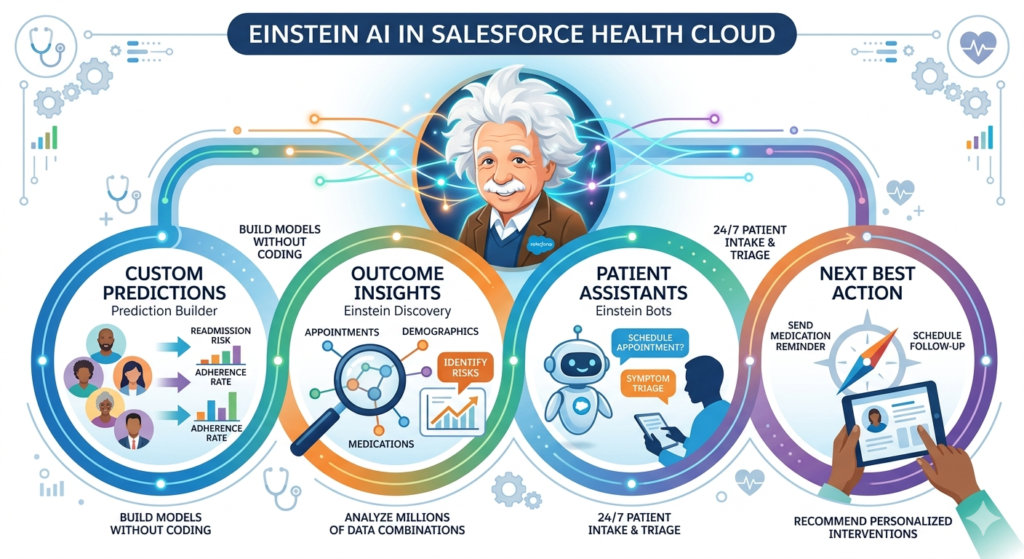
Core Einstein Components Relevant to Patient Care
Einstein Prediction Builder allows healthcare organizations to create custom AI models without coding. A care management team can build models predicting hospital readmissions, medication non-adherence, or disease progression by simply selecting relevant patient data fields and defining outcome criteria.
Einstein Discovery automatically analyzes millions of patient data combinations to surface the factors most strongly correlating with specific outcomes. For instance, it might reveal that patients with diabetes who miss two consecutive appointments and live more than 15 miles from their provider face 73% higher risk of diabetic complications—an insight enabling targeted intervention.
Einstein Bots powered by Natural Language Processing (NLP) can conduct patient intake, triage symptoms, schedule appointments, and answer common questions 24/7, freeing care coordinators for complex cases requiring human judgment.
Einstein Next Best Action recommends specific interventions for individual patients by evaluating their complete health profile against clinical protocols, resource availability, and predicted effectiveness.
Einstein Language extracts meaningful clinical information from unstructured notes, patient messages, and referral documents, converting narrative text into structured, actionable data.
The Health Cloud Data Foundation
For AI to function effectively, it requires comprehensive, clean, and connected data. Health Cloud consolidates disparate information sources into unified patient profiles:
- Electronic Health Records (EHR) integration via HL7 FHIR standards
- Claims data revealing utilization patterns and cost drivers
- Social determinants of health (housing stability, food security, transportation access)
- Patient-reported outcomes through mobile apps and portals
- Wearable device data for continuous monitoring
- Care team communications documenting intervention history
Einstein algorithms consume this holistic patient view, identifying correlations across clinical, behavioral, and environmental factors that traditional analytics miss.
Key AI Capabilities for Predictive Patient Care
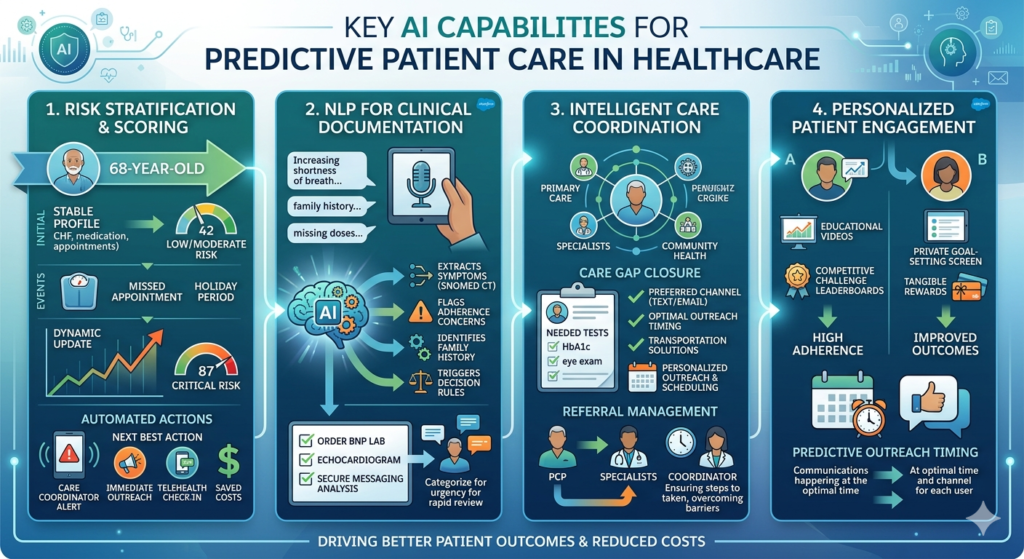
1. Risk Stratification and Predictive Scoring
Risk stratification represents perhaps the highest-impact application of AI in Salesforce Health Cloud. Healthcare organizations manage thousands or millions of patients with finite care management resources. AI-powered risk scoring identifies which patients need proactive intervention most urgently.
How It Works in Practice:
Einstein analyzes each patient’s comprehensive health profile—diagnoses, medications, lab results, hospitalization history, appointment attendance, insurance coverage gaps, and social determinants. The system assigns dynamic risk scores that update continuously as new information arrives.
A 68-year-old patient with congestive heart failure might receive a risk score of 42 (moderate) based on stable condition and regular appointments. When the patient’s connected scale detects a sudden 5-pound weight gain over three days (indicating fluid retention), misses a scheduled cardiology appointment, and the algorithm notes an upcoming holiday period (when many patients lapse on medication), the risk score automatically elevates to 87 (critical).
This triggers an automated workflow: the care coordinator receives a prioritized alert, Einstein suggests immediate outreach, and the next best action recommendation proposes scheduling a same-day telehealth check-in to assess symptoms and adjust diuretics before hospitalization becomes necessary.
Real-World Impact:
A 450-bed hospital system implemented Einstein risk scoring for heart failure patients. By identifying the top 15% highest-risk patients for intensive care management, they reduced 30-day readmissions by 31% in that cohort over six months—saving approximately $2.8 million in Medicare penalties and avoided costs while demonstrably improving patient outcomes.
2. Natural Language Processing for Clinical Documentation
Clinical documentation consumes 30-40% of many providers’ time and often contains critical information locked in unstructured text. Einstein’s NLP capabilities extract actionable intelligence from narrative notes, patient messages, and referral documents.
Practical Application:
When a primary care provider dictates: “Patient reports increasing shortness of breath on exertion, difficulty sleeping flat, and bilateral ankle swelling over the past two weeks. Family history significant for cardiomyopathy. Currently takes lisinopril 10mg but admits missing doses ‘a few times’ last month.”
Einstein NLP automatically:
- Extracts symptoms and codes them to standardized terminologies (SNOMED CT)
- Flags medication adherence concerns
- Identifies relevant family history
- Updates the patient’s symptom timeline
- Triggers clinical decision support rules for potential heart failure exacerbation
- Suggests ordering BNP lab test and echocardiogram based on clinical guidelines
This happens instantly upon note completion, creating structured data that feeds predictive models while reducing manual data entry burden.
Secure Messaging Analysis:
Einstein also analyzes patient portal messages for urgency and clinical significance. When a patient messages “I think I might be running a fever and my surgical incision looks a little red,” NLP categorizes this as potentially urgent, extracts the relevant symptoms, flags the recent surgical history, and routes it for rapid nurse review rather than the standard 48-hour response queue.
3. Intelligent Care Coordination and Workflow Automation
Coordinating care across multiple providers, specialists, and settings represents a persistent healthcare challenge. AI in Salesforce Health Cloud orchestrates this complexity through intelligent automation that adapts to individual patient contexts.
Care Gap Closure:
Einstein identifies gaps between evidence-based care guidelines and actual patient care. For a patient with diabetes, the system recognizes they’re overdue for annual eye exam, HbA1c testing, and foot examination. Rather than generic reminders, Einstein evaluates:
- Patient’s preferred communication channel (text vs. email vs. phone)
- Optimal outreach timing based on historical response patterns
- Proximity to in-network providers offering required services
- Transportation barriers that might prevent appointment attendance
- Insurance authorization requirements
The system then orchestrates a personalized outreach sequence: sends a text message on Tuesday morning (when this patient historically responds best) with direct scheduling links to nearby ophthalmologists accepting new patients, arranges transportation through a community health worker for those with mobility challenges, and auto-generates prior authorization requests where needed.
Referral Management:
When a primary care provider refers a patient to a cardiologist, Einstein monitors the referral lifecycle. If the patient hasn’t scheduled the cardiology appointment within one week, the system triggers care coordinator outreach to identify and resolve barriers—perhaps the specialist’s office never received the referral, the patient doesn’t understand why they need the specialist, or they lack transportation.
4. Personalized Patient Engagement and Interventions
Generic patient engagement programs achieve modest results because they ignore individual circumstances, preferences, and readiness to change. AI enables true personalization at scale.
Behavioral Pattern Recognition:
Einstein analyzes each patient’s engagement history to determine optimal intervention strategies. For chronic disease management programs, the system identifies:
- Which educational content formats individuals engage with (video, text, interactive tools)
- What times of day patients typically interact with health apps
- Which behavior change techniques prove most effective for specific personality profiles
- Warning signs of program disengagement before dropout occurs
A diabetes management program might discover that Patient A responds well to competitive challenges and social comparison (leaderboards, peer support groups), while Patient B prefers private goal-setting with tangible rewards. Einstein automatically customizes program delivery for each individual, dramatically improving adherence and outcomes.
Predictive Outreach Timing:
Rather than batch-processing appointment reminders at arbitrary times, Einstein predicts optimal outreach moments for each patient. Analysis might reveal that a particular patient is 40% more likely to confirm appointments when contacted on Thursday afternoons versus Monday mornings, and prefers text messages over phone calls by a 3:1 margin. The system automatically schedules communications accordingly.
Real-World Use Cases: AI in Salesforce Health Cloud Implementation
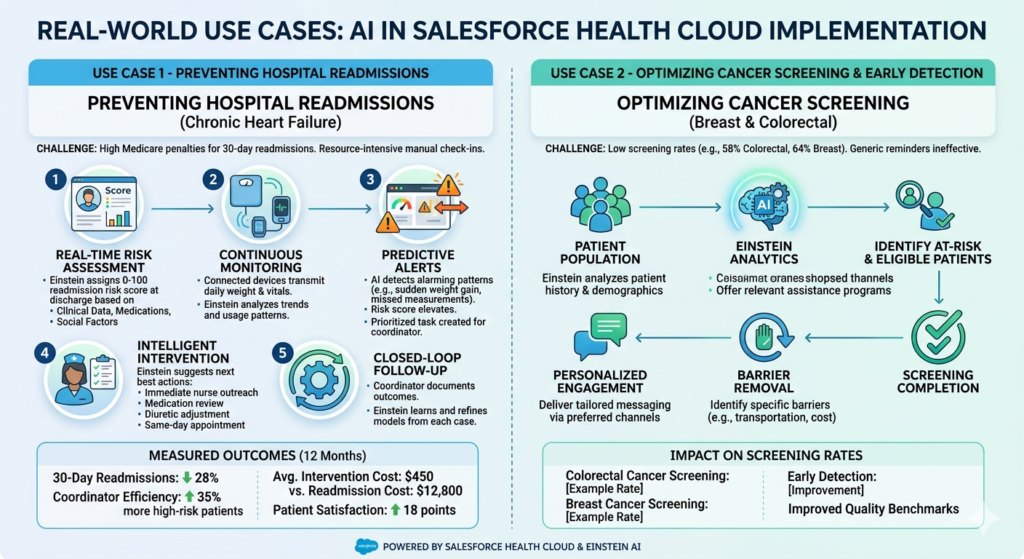
Use Case 1: Preventing Hospital Readmissions for Chronic Heart Failure
The Challenge:
A large integrated delivery network faced significant Medicare penalties for excessive 30-day readmissions among heart failure patients. Traditional care management approaches—calling all recently discharged patients to check symptoms—proved resource-intensive and missed many patients who deteriorated between weekly check-ins.
The AI-Powered Solution:
The organization implemented an Einstein-powered predictive readmission prevention program in Health Cloud with the following workflow:
Step 1: Real-Time Risk Assessment
Upon discharge, Einstein assigns each heart failure patient a readmission risk score (0-100) based on:
- Clinical factors: ejection fraction, NT-proBNP levels, comorbidities, number of prior hospitalizations
- Medication complexity: number of prescriptions, changes from previous regimen
- Social determinants: living alone, food insecurity, transportation barriers, health literacy scores
- Behavioral patterns: historical appointment adherence, medication refill patterns
Step 2: Continuous Monitoring
Patients receive connected weight scales and pulse oximeters that automatically transmit data to Health Cloud. Einstein analyzes:
- Daily weight trends (sudden gain indicating fluid retention)
- Heart rate variability patterns
- Device usage consistency (non-use itself being a risk signal)
Step 3: Predictive Alerts
When Einstein detects concerning patterns—a 72-year-old patient’s weight increased 4 pounds in two days, they haven’t taken weight measurements in three consecutive days (suggesting worsening fatigue), and their medication refill is overdue—the system automatically:
- Elevates risk score from 45 to 89
- Creates a prioritized task for the care coordinator
- Prepares next best action recommendations
Step 4: Intelligent Intervention
Einstein suggests specific actions ranked by predicted effectiveness:
- Immediate nurse outreach to assess symptoms (phone or video visit)
- Medication reconciliation to identify adherence barriers
- Diuretic dose adjustment protocol
- Home health visit if patient reports severe symptoms
- Same-day clinic appointment scheduling with cardiology nurse practitioner
Step 5: Closed-Loop Follow-Up
The care coordinator executes interventions, documenting outcomes in Health Cloud. Einstein learns from each case—when interventions successfully prevented readmission versus when hospitalization still occurred—continuously refining its predictive models and recommendations.
Measured Outcomes:
- 30-day heart failure readmissions decreased 28% over 12 months
- Care coordinator efficiency improved—they managed 35% more high-risk patients with the same staffing
- Average intervention cost per prevented readmission: $450
- Average readmission cost avoided: $12,800
- Patient satisfaction scores increased 18 points due to proactive, personalized care
Use Case 2: Optimizing Cancer Screening and Early Detection
The Challenge:
A regional health system struggled with low cancer screening rates—only 58% of eligible patients completed colorectal cancer screening, and 64% completed breast cancer screening, well below national quality benchmarks. Traditional reminder campaigns yielded minimal improvement because they didn’t address the specific barriers each patient faced.
The AI-Powered Solution:
Step 1: Eligibility Intelligence
Einstein automatically identifies screening-eligible patients by analyzing:
- Age and gender criteria for various cancer screenings
- Family history indicating higher-risk populations requiring earlier/more frequent screening
- Previous screening dates and results
- Current symptoms or clinical findings suggesting screening urgency
The system maintains a dynamic “screening due” registry that updates daily as patients age into eligibility, time intervals elapse, or new risk factors emerge.
Step 2: Barrier Prediction
For each eligible patient, Einstein Discovery analyzes historical data across the population to predict which specific barriers likely prevent screening completion:
- Clinical anxiety: Patients who’ve previously canceled procedures or expressed fear in clinical notes
- Logistical barriers: Lack of transportation, inflexible work schedules, childcare challenges
- Knowledge gaps: Patients who’ve never received education about screening importance
- Access issues: Lack of insurance coverage, prefer providers not in network
- Cultural factors: Language barriers, cultural beliefs about preventive care, distrust of healthcare system
Step 3: Personalized Intervention Design
Based on predicted barriers, Einstein recommends tailored outreach strategies:
For patients with clinical anxiety:
- Educational content emphasizing comfort measures and sedation options
- Testimonial videos from similar patients who completed screening
- Offer for pre-procedure counseling with nurse navigator
For patients with transportation barriers:
- Information about free transportation services
- Mobile screening unit locations and schedules
- At-home screening options (FIT kits for colorectal cancer)
For patients with knowledge gaps:
- Culturally appropriate educational materials in preferred language
- Explanation of insurance coverage (most preventive screenings are $0 copay)
- Physician video message emphasizing personal risk factors
Step 4: Optimal Outreach Orchestration
Einstein determines the best communication channel, timing, and messenger for each patient:
- Some respond better to physician outreach; others prefer nurse navigators
- Optimal contact days and times based on historical response patterns
- Preferred channels (text, email, phone, patient portal)
- Whether peer testimonials or clinical authority messaging proves more persuasive
Step 5: Engagement Monitoring and Adaptive Follow-Up
The system tracks who opens messages, clicks scheduling links, schedules appointments, and completes screenings. When patients don’t respond to initial outreach, Einstein adapts:
- Tries alternative communication channels
- Escalates to personal phone call from care team member
- Addresses different potential barriers in subsequent messages
- Identifies when continued outreach becomes counterproductive (predictive unsubscribe risk)
Measured Outcomes:
- Colorectal cancer screening rates increased from 58% to 79% over 18 months
- Breast cancer screening rates increased from 64% to 81%
- Three early-stage cancers detected that likely would have progressed to later stages without intervention
- Cost per additional screening completed: $42 (vs. $890 for late-stage cancer treatment)
- Patient complaints about “annoying reminders” decreased 35% due to personalized, relevant messaging
Use Case 3: Managing High-Risk Pregnancy Outcomes
The Challenge:
A maternal-fetal medicine practice needed to identify high-risk pregnancies requiring specialized monitoring and intervention. Traditional risk assessment occurred only at initial prenatal visits and didn’t account for evolving complications or social factors that emerged during pregnancy.
The AI-Powered Solution:
Step 1: Comprehensive Risk Modeling
Einstein creates a dynamic pregnancy risk score for each patient, continuously updated throughout gestation based on:
Clinical factors:
- Pre-existing conditions (diabetes, hypertension, autoimmune disorders)
- Pregnancy complications (gestational diabetes, preeclampsia, placental issues)
- Previous pregnancy outcomes (preterm birth, stillbirth, cesarean delivery)
- Current pregnancy progress (fetal growth measurements, lab abnormalities)
Social determinants:
- Housing instability
- Food insecurity
- Domestic violence screening results
- Substance use concerns
- Inadequate prenatal care utilization
- Transportation barriers to appointments
Behavioral patterns:
- Appointment adherence
- Medication compliance
- Engagement with prenatal education
Step 2: Predictive Alerting for Complications
The system identifies early warning patterns predicting specific complications:
For preterm labor risk:
- Previous preterm delivery + current cervical length shortening + missed appointments
- Triggers recommendation for cervical cerclage consultation and increased monitoring
For gestational diabetes progression:
- Borderline glucose tolerance test + excessive weight gain + family history
- Triggers early glucose monitoring and nutritional counseling before diagnosis
For postpartum depression risk:
- History of depression + limited social support + unplanned pregnancy
- Triggers enhanced mental health screening and support services
Step 3: Care Coordination Across Multiple Touchpoints
High-risk pregnancies involve multiple specialists (maternal-fetal medicine, endocrinology, cardiology), social services, and support programs. Einstein orchestrates this complexity:
- Automatically schedules specialist referrals based on risk factors
- Ensures recommended testing occurs at appropriate gestational ages
- Tracks completion of all care plan elements
- Identifies gaps when recommended interventions don’t occur
- Facilitates communication among all care team members through shared care plans
Step 4: Intelligent Patient Support
Einstein Bots provide 24/7 patient access for questions and symptom triage:
Patient: “I’m 32 weeks and having contractions every 15 minutes for the past hour.”
Bot response: “I understand you’re experiencing regular contractions. At 32 weeks, this requires immediate evaluation. I see you’re a patient of Dr. Chen’s practice. I can help you:
- Contact labor and delivery now for immediate evaluation (RECOMMENDED)
- Schedule an urgent office visit today
- Speak with the on-call nurse
Which would you prefer?”
The system documents the interaction, updates the patient’s record, and alerts the clinical team about the potential preterm labor case.
Step 5: Postpartum Transition
Risk doesn’t end at delivery. Einstein identifies patients at high risk for postpartum complications:
- Postpartum depression screening based on risk factors
- Medication adherence monitoring (especially for chronic conditions like diabetes or hypertension)
- Infant care appointment attendance
- Contraception counseling for those with contraindicated future pregnancies
Measured Outcomes:
- Preterm births (<37 weeks) decreased 24% among high-risk population
- NICU admissions reduced 19%
- Postpartum depression diagnosis and treatment initiation increased 43% due to proactive screening
- Patient satisfaction with care coordination improved significantly (NPS +28 points)
- Average cost savings per prevented preterm birth: $47,000
Use Case 4: Predictive Population Health for Chronic Disease Management
The Challenge:
A large accountable care organization (ACO) managed 85,000 patients with chronic conditions (diabetes, hypertension, COPD, asthma) across 200+ primary care providers. Traditional quality improvement efforts—providing physicians with quarterly reports of their diabetic patients with elevated HbA1c—proved ineffective because doctors lacked time to systematically reach out to poorly controlled patients, and the reports were outdated by the time they arrived.
The AI-Powered Solution:
Step 1: Real-Time Clinical Surveillance
Einstein continuously monitors all patients with chronic conditions, analyzing:
- Lab results compared to evidence-based targets (HbA1c <7%, LDL <100, blood pressure <140/90)
- Medication adherence patterns from pharmacy claims
- Appointment attendance and care plan completion
- Emergency department visits and hospitalizations
- Patient-reported symptoms and quality of life measures
The system identifies patients whose chronic conditions are deteriorating before clinical crises occur.
Step 2: Predictive Complication Modeling
For each patient, Einstein predicts likelihood of specific complications:
Diabetes patients:
- Probability of diabetic retinopathy, neuropathy, or nephropathy development
- Risk of hypoglycemic events requiring emergency care
- Likelihood of progressing to insulin-dependent status
COPD patients:
- Probability of exacerbation requiring hospitalization in next 3 months
- Risk of respiratory failure requiring intubation
- Likelihood of benefiting from pulmonary rehabilitation
Step 3: Care Prioritization and Resource Allocation
The ACO employs 40 care managers who can’t possibly reach all 85,000 chronic disease patients. Einstein solves this resource allocation challenge by:
- Ranking patients by combination of clinical risk and intervention responsiveness
- Identifying patients most likely to benefit from care management (not just highest risk)
- Matching patients to care managers based on expertise, language, and previous relationship effectiveness
- Dynamically adjusting caseloads as patient conditions change
A patient might have high clinical risk (diabetes with HbA1c of 10.2%) but low intervention responsiveness (has ignored outreach for past year, doesn’t attend appointments, doesn’t refill medications). Einstein prioritizes a moderately high-risk patient with better engagement indicators for immediate care management while routing the highly resistant patient to a motivational interviewing specialist.
Step 4: Precision Intervention Design
For prioritized patients, Einstein recommends specific interventions based on predicted effectiveness:
For a diabetic patient with poor control:
- Root cause analysis: Medication non-adherence due to cost, not lack of prescription
- Recommended intervention: Switch to formulary-preferred, lower-cost alternative + prescription assistance program enrollment
- Predicted outcome: 78% probability of HbA1c improvement within 3 months
- Alternative intervention if first fails: Simplified medication regimen (once-daily vs. multiple daily doses)
Step 5: Provider Decision Support
Rather than overwhelming physicians with reports, Einstein delivers actionable intelligence at the point of care:
When Dr. Smith opens a diabetic patient’s chart before an appointment, an Einstein insight appears:
“This patient’s pharmacy data shows they haven’t refilled metformin in 4 months. Three similar patients with this pattern achieved HbA1c reduction averaging 1.8% when switched to once-weekly semaglutide. Consider discussing this option today.”
Step 6: Outcome Learning and Model Refinement
Einstein continuously evaluates which interventions actually improved outcomes for which patient profiles:
- Did medication switches improve adherence?
- Did care manager outreach result in behavior change?
- Which patient characteristics predicted intervention success?
The system refines its recommendations based on this feedback loop, becoming more accurate over time.
Measured Outcomes:
- Overall diabetes control (HbA1c <8%) improved from 68% to 81% of population
- Hypertension control increased from 62% to 77%
- COPD exacerbations requiring hospitalization decreased 34%
- Medicare Shared Savings Program performance: earned $8.2M in shared savings vs. $2.1M previous year
- Care manager productivity: managed 45% more patients at higher complexity without additional staffing
- Physician satisfaction increased—they received relevant, actionable information instead of overwhelming reports
Use Case 5: Mental Health Crisis Prevention and Intervention
The Challenge:
A behavioral health network struggled to identify patients at elevated suicide risk between appointments. Most patients who died by suicide had no obvious warning signs during their last clinical encounter, but retrospective analysis often revealed subtle behavioral changes—appointment cancellations, medication non-adherence, decreased engagement—that weren’t recognized as crisis indicators in real-time.
The AI-Powered Solution:
Step 1: Comprehensive Risk Assessment
Einstein analyzes multiple data streams to calculate dynamic suicide risk scores:
Clinical data:
- Diagnosis severity and complexity
- Recent psychiatric hospitalizations
- Medication changes (especially antidepressant discontinuation)
- Substance use comorbidities
- History of self-harm or previous attempts
Behavioral signals:
- Appointment cancellation patterns
- Medication refill gaps
- Decreased engagement with therapy homework or mobile app tools
- Changes in patient portal activity (sudden increase in desperate-sounding messages or complete disengagement)
Environmental factors:
- Recent life stressors (documented job loss, relationship changes, housing instability)
- Social isolation indicators
- Anniversary dates of traumatic events or losses
- Seasonal patterns (some patients deteriorate predictably during specific months)
Step 2: Natural Language Processing for Warning Signs
Einstein analyzes unstructured data for crisis indicators:
Therapist notes: “Patient seemed more withdrawn than usual. Mentioned feeling like ‘a burden’ to family. Made oblique reference to ‘not being around much longer’ but denied suicidal ideation when directly asked.”
Einstein flags indirect language patterns associated with suicide risk that might be overlooked in busy clinical workflows, creating alerts for clinical review.
Patient portal messages: “I don’t think the medication is helping anymore. Nothing seems to help. I’m just so tired of fighting.”
NLP detects hopelessness language patterns and escalates the message for immediate clinical review rather than routine response timeline.
Step 3: Predictive Crisis Alerting
When risk scores elevate above threshold or concerning patterns emerge, Einstein generates tiered alerts:
Moderate concern (risk score 60-79):
- Alert assigned therapist for phone check-in within 24 hours
- Suggest offering earlier appointment if patient agrees
- Document increased monitoring plan
High concern (risk score 80-89):
- Alert assigned therapist and psychiatric prescriber immediately
- Recommend same-day safety assessment (in-person or telehealth)
- Prepare safety planning resources
- Consider intensive outpatient program or partial hospitalization
Critical concern (risk score 90-100):
- Immediate multi-disciplinary alert (therapist, psychiatrist, crisis team)
- Protocol for immediate safety contact (therapist calls patient directly)
- Mobile crisis team dispatch if patient can’t be reached or acknowledges active plan
- Family/emergency contact outreach if appropriate and authorized
Step 4: Intelligent Safety Planning
For patients identified at elevated risk, Einstein helps create personalized safety plans by:
- Identifying this patient’s specific warning signs based on historical patterns
- Recommending coping strategies that worked for this individual previously
- Populating crisis resources based on patient location and preferences
- Scheduling automated check-ins via preferred communication channel
- Engaging support system (with patient consent)
Step 5: Continuous Monitoring and Support
Einstein Bots provide between-session support:
Patient (via text, 2 AM): “Can’t sleep. Keep thinking about dying.”
Bot response: “I’m concerned about what you’re sharing. Your safety is most important.
If you’re thinking about suicide right now, please:
• Call 988 Suicide & Crisis Lifeline (24/7 support)
• Text ‘HELLO’ to 741741 for Crisis Text Line
• Go to your nearest emergency room
• Call 911 if you’re in immediate danger
Would you like me to notify your therapist, Dr. Martinez, about how you’re feeling?”
The interaction is documented, alerts the clinical team, and provides immediate resources while maintaining therapeutic connection.
Step 6: Outcome Analysis and Model Refinement
The system tracks:
- Which risk indicators most accurately predicted actual crises
- Which interventions successfully de-escalated high-risk situations
- False positive rates (alerts that didn’t result in actual crisis)
- Missed cases (crises that occurred without triggering alerts)
Einstein continuously refines risk algorithms based on this feedback, improving sensitivity and specificity over time.
Measured Outcomes:
- Identification of high-risk patients increased 67% (catching concerning patterns earlier)
- Completed suicides among active patients decreased from 4 per year to 1 over 24-month period
- Successful crisis interventions (prevented hospitalizations/attempts): 43 documented cases
- Therapist early warning of deteriorating patients improved clinical outcomes
- Reduced liability risk through documented, proactive monitoring systems
- Patient-reported sense of support between sessions increased significantly
Step-by-Step Implementation Guide: Building Your AI-Powered Predictive Care Program
Phase 1: Foundation and Assessment (Weeks 1-4)
Step 1: Define Your Predictive Care Objectives
Begin with specific, measurable goals rather than vague aspirations to “use AI.” Examples:
- Reduce heart failure readmissions by 20% within 12 months
- Increase colorectal cancer screening rates from 58% to 75%
- Identify 90% of diabetic patients at risk for complications before they occur
- Decrease emergency department utilization among chronic disease population by 15%
Step 2: Assess Data Readiness
AI quality depends entirely on data quality. Audit your current state:
Data completeness:
- What percentage of patient records contain structured diagnosis codes?
- Are social determinants of health documented systematically?
- Do you capture medication adherence data beyond prescriptions written?
- Are patient-reported outcomes collected consistently?
Data connectivity:
- Which systems contain relevant patient data (EHR, claims, labs, pharmacy, patient portal)?
- Do existing integration standards exist (HL7 FHIR)?
- What data refresh frequency can you achieve (real-time, daily, weekly)?
Data quality:
- Error rates in key fields
- Standardization of clinical terminologies
- Duplicate patient records
- Data governance policies and stewardship
Step 3: Identify Initial Use Case
Don’t attempt to transform all care processes simultaneously. Select one high-impact use case that:
- Addresses a significant clinical or financial pain point
- Has available data to support predictive modeling
- Involves a defined patient population (not “all patients”)
- Has executive sponsorship and engaged clinical champions
- Can demonstrate measurable outcomes within 6-12 months
Step 4: Assemble Your Implementation Team
Successful AI implementation requires diverse expertise:
- Clinical lead: Physician or advanced practice provider who understands workflows and will champion adoption
- Care operations lead: Manager of care coordinators/navigators who will use the system daily
- Salesforce administrator: Technical expert on Health Cloud configuration
- Data analyst: Expertise in healthcare data, predictive modeling, and outcome measurement
- Integration specialist: Manages connections between Health Cloud and source systems
- Compliance/legal advisor: Ensures HIPAA compliance, consent management, algorithm governance
- Project manager: Coordinates timeline, resources, and stakeholder communications
Phase 2: Data Integration and Model Development (Weeks 5-12)
Step 5: Establish Data Connections
Integrate relevant data sources into Health Cloud:
EHR Integration:
Most organizations use Mirth Connect, Rhapsody, or similar integration engines to:
- Pull patient demographics, diagnoses, medications, procedures, vital signs, lab results
- Map HL7 messages to Health Cloud objects (Patient, Care Plan, Clinical Service Request, etc.)
- Establish bi-directional communication where appropriate
Claims Data:
Claims reveal utilization patterns invisible in clinical data alone:
- Emergency department visits
- Hospital admissions and readmissions
- Specialist referrals and adherence
- Medication fills (actual adherence vs. prescribed)
- Cost and coverage information
Patient-Generated Data:
Increasingly critical for predictive models:
- Patient portal messages and symptom reports
- Wearable device data (activity, heart rate, sleep, weight)
- Patient-reported outcome measures
- Appointment scheduling and attendance
Social Determinants:
Often the strongest predictors of outcomes:
- Housing stability screening
- Food insecurity assessments
- Transportation access
- Health literacy measures
- Social support networks
Step 6: Clean and Standardize Data
Apply data quality processes:
- Deduplicate patient records using probabilistic matching algorithms
- Standardize clinical terminologies (ICD-10, SNOMED CT, LOINC, RxNorm)
- Validate data accuracy through sampling and clinical review
- Establish data governance policies for ongoing quality
Step 7: Build Your First Predictive Model Using Einstein Prediction Builder
Let’s use hospital readmission prediction as a concrete example:
Define the prediction:
“Will this patient be readmitted within 30 days of discharge?”
Select the object:
Patient (or a custom object like “Hospital Discharge”)
Choose your outcome field:
“Readmitted_30_Days__c” (Boolean: Yes/No)
Select predictor fields (Einstein analyzes these to build the model):
- Demographics: Age, gender
- Clinical: Primary diagnosis, comorbidity count, length of stay, ICU admission, previous hospitalizations
- Medications: Number of prescriptions at discharge, medication changes from admission
- Social: Lives alone, transportation barriers, health literacy score
- Behavioral: Historical appointment adherence rate, medication fill adherence
Set filters to define your training population:
- Include only adult discharges (age ≥18)
- Exclude obstetric, psychiatric, and hospice discharges (different readmission dynamics)
- Minimum 2 years of historical data
Train the model:
Einstein analyzes your historical data, identifying which factors most strongly predict readmissions. The platform automatically:
- Splits data into training and validation sets
- Tests multiple algorithm approaches
- Evaluates model accuracy (sensitivity, specificity, positive predictive value)
- Ranks predictor importance
Review model performance:
Einstein presents model quality metrics:
- “This model correctly predicts readmissions 78% of the time”
- “Top predictive factors: Previous hospitalizations (32% influence), Number of medications at discharge (21%), Lives alone (14%)”
If accuracy is insufficient, iterate by:
- Adding additional predictor fields
- Increasing training data volume
- Segmenting the population (separate models for heart failure vs. pneumonia vs. surgery)
Step 8: Configure Einstein Discovery for Deep Insights
While Prediction Builder creates models for specific outcomes, Einstein Discovery explores your data to surface unexpected insights:
Upload a dataset of diabetic patients with fields including:
- Demographics, clinical measures (HbA1c, BMI, comorbidities), social factors, care engagement metrics, and outcome (achieved HbA1c <7% in past year: Yes/No)
Einstein Discovery analyzes millions of combinations and might surface insights like:
“Patients with HbA1c >9% who attend group diabetes education classes are 2.3x more likely to achieve control than those receiving only individual counseling—but only if they attend at least 4 sessions. Patients attending 1-2 sessions show no improvement over no education.”
This insight enables you to:
- Prioritize group education class offerings
- Implement minimum attendance tracking
- Redesign individual counseling approach for those who prefer it
Phase 3: Workflow Integration and Automation (Weeks 13-16)
Step 9: Design Care Team Workflows
AI predictions are worthless unless they trigger appropriate actions. Map how predictions will integrate into daily workflows:
For care coordinators:
- Morning dashboard shows prioritized patient list ranked by Einstein risk scores
- Clicking any patient shows risk factors, predicted outcomes, and next best actions
- Workflow guides document interventions and outcomes for continuous learning
For physicians:
- Einstein insights surface within EHR at point of care
- Alerts appear non-intrusively (avoid alert fatigue)
- Recommendations include clinical evidence and patient-specific reasoning
For front desk staff:
- Scheduling system flags high-risk patients who need priority appointment slots
- Automatically books longer appointment times for complex patients
- Prompts to offer telehealth alternatives for patients with transportation barriers
Step 10: Configure Einstein Next Best Action
Next Best Action translates predictions into specific recommendations:
Create recommendation strategies:
For a patient with elevated readmission risk score:
IF risk score >80 AND primary diagnosis = heart failure:
- RECOMMEND: Schedule 48-hour post-discharge phone call with cardiology nurse
- RECOMMEND: Enroll in remote monitoring program with daily weight checks
- RECOMMEND: Home health visit within 3 days
IF risk score >80 AND medication count >10:
- RECOMMEND: Pharmacist medication reconciliation and simplification consultation
- RECOMMEND: Medication synchronization (all refills due on same day)
IF risk score >80 AND lives alone:
- RECOMMEND: Social work assessment for support services
- RECOMMEND: Caregiver education and involvement
- RECOMMEND: Meal delivery program enrollment
Rank recommendations by predicted impact (Einstein can help estimate effectiveness based on historical outcomes)
Configure display within care coordinator workspaces for seamless workflow
Step 11: Implement Intelligent Automation
Automate routine actions triggered by predictions:
Automated outreach:
When a patient’s chronic disease risk score elevates:
- System automatically sends personalized education content
- Schedules proactive care coordinator phone call
- Creates draft appointment for physician review/approval
Automated care gap alerts:
When Einstein identifies screening due:
- Sends patient reminder via preferred channel
- Provides direct scheduling link
- Alerts care team if patient doesn’t schedule within 2 weeks
Automated documentation:
- Einstein Bot interactions automatically update patient record
- Risk score changes generate audit trail
- Intervention outcomes feed back to improve predictions
Step 12: Configure Einstein Bots for Patient Interaction
Design conversational flows for common scenarios:
Symptom triage bot:
Patient inputs symptoms → Bot asks clarifying questions → Assesses urgency using clinical protocols → Routes to appropriate care level (self-care, appointment needed, urgent care, emergency)
Appointment scheduling bot:
Patient requests appointment → Bot checks availability → Considers patient-specific factors (high-risk patients offered sooner slots, transportation barriers trigger telehealth option) → Books appointment and sends confirmation
Medication refill bot:
Patient requests refill → Bot verifies medication and prescriber → Checks for required follow-up (some medications require recent lab work) → Processes routine refills or alerts clinical team if issues
Phase 4: Testing and Validation (Weeks 17-20)
Step 13: Conduct Model Validation
Before deploying predictions to guide patient care, validate rigorously:
Retrospective testing:
Apply your readmission prediction model to patients discharged 6 months ago. Compare predictions against actual outcomes:
- Did the model accurately identify who was readmitted?
- Were high-risk patients truly higher risk, or did the model misclassify?
- Calculate sensitivity (% of actual readmissions predicted), specificity (% of non-readmissions correctly identified), positive predictive value (% of high-risk predictions that were accurate)
Prospective silent testing:
Run the model in production for 30 days without care teams acting on predictions. Track:
- Model predictions
- Actual outcomes
- Any concerning patterns (e.g., systematically underpredicting risk for specific demographic groups)
Bias and equity analysis:
Ensure the model performs equitably across populations:
- Does it perform equally well for different racial/ethnic groups?
- Are there gender disparities in prediction accuracy?
- Does it inadvertently disadvantage socioeconomically vulnerable populations?
Address any identified biases before clinical deployment.
Step 14: User Acceptance Testing
Engage actual end users in testing:
Care coordinators:
- Can they efficiently navigate prioritized patient lists?
- Are next best action recommendations clear and actionable?
- Does the system integrate smoothly with existing workflows or create friction?
Physicians:
- Do alerts provide value or create annoyance?
- Is clinical reasoning behind recommendations transparent?
- Can they easily document outcomes to improve future predictions?
IT and compliance:
- Does the system maintain HIPAA compliance?
- Are audit trails sufficient?
- Is performance acceptable (page load times, system responsiveness)?
Iterate based on feedback before broad rollout.
Step 15: Develop Training Materials and Support
Create role-specific training:
For clinical staff:
- How to interpret risk scores and Einstein insights
- When to follow AI recommendations vs. apply clinical judgment
- How to document interventions and outcomes
- Understanding model limitations (AI augments, doesn’t replace, clinical expertise)
For patients (where appropriate):
- How their data is being used to improve care
- Privacy protections and consent
- How to engage with AI-powered tools (bots, remote monitoring)
Phase 5: Deployment and Optimization (Weeks 21-24 and Ongoing)
Step 16: Phased Rollout
Deploy incrementally rather than organization-wide simultaneously:
Week 21-22: Pilot with single care team
- 2-3 care coordinators using the system with their full patient panels
- Daily check-ins to troubleshoot issues
- Rapid iteration on workflow refinements
Week 23-24: Expand to additional teams
- Incorporate lessons from pilot
- Broader training rollout
- Establish ongoing support model
Month 4-6: Full deployment
- All care teams using AI-powered workflows
- Standardized processes and governance
- Regular optimization cycles
Step 17: Establish Continuous Learning Processes
AI improves with use—if you establish feedback loops:
Outcome documentation:
Ensure care teams document intervention results:
- Did the predicted high-risk patient actually experience the adverse outcome?
- Did the recommended intervention prevent it?
- If intervention failed, what alternative approach worked?
Model retraining:
Retrain Einstein models quarterly with updated data:
- Incorporates new patients and recent outcomes
- Adapts to changes in care delivery
- Maintains accuracy as population characteristics evolve
Insight review meetings:
Monthly multidisciplinary meetings to review:
- Einstein Discovery insights from recent data
- Model performance trends
- Workflow optimization opportunities
- New use case possibilities
Step 18: Measure and Communicate Impact
Track both clinical and operational metrics:
Clinical outcomes:
- Primary target (e.g., readmission rate change)
- Secondary measures (ED utilization, medication adherence, screening completion)
- Patient experience and satisfaction
Operational metrics:
- Care coordinator productivity (patients managed per FTE)
- Intervention efficiency (cost per intervention vs. cost of avoided event)
- Workflow time savings
- Alert accuracy (% requiring action vs. false alarms)
Financial impact:
- Avoided costs from prevented adverse events
- Shared savings program performance
- Quality incentive achievement
- ROI on implementation investment
Share results broadly:
- Clinical staff (celebrate successes, engage in problem-solving)
- Executive leadership (demonstrate value, secure ongoing support)
- Board (strategic impact)
- Patients (transparency about how AI improves their care)
Challenges and Limitations: Navigating the Reality of Healthcare AI
Data Quality and Interoperability Challenges
The promise of AI analytics exceeds reality when data is incomplete, inaccurate, or inaccessible. Healthcare data remains fragmented across EHRs, claims systems, pharmacies, labs, and patient-generated sources. Many organizations discover during implementation that seemingly simple data elements are actually inconsistent, missing, or unreliable.
Practical challenges include:
- Diagnosis coding inconsistencies: A patient’s diabetes might be coded as E11.9 by one provider, Type 2 diabetes mellitus without complications by another (narrative text), and not documented at all in specialist notes focusing on other issues
- Medication reconciliation gaps: Prescribed medications don’t reflect what patients actually take; pharmacy fill data shows prescriptions filled but not whether they were consumed
- Social determinant documentation: Critical predictive factors (housing stability, food insecurity, health literacy) are often captured in narrative notes—if at all—rather than structured, queryable fields
- Care occurring outside your system: Patients see multiple healthcare organizations; predictions based only on your organization’s data miss critical context
Mitigation strategies:
- Invest in data quality improvement before AI implementation—garbage in, garbage out applies absolutely
- Implement standardized screening tools for social determinants with discrete data capture
- Utilize Einstein NLP to extract information from unstructured notes, converting narrative to structured data
- Pursue health information exchange connections to access external care data
- Design AI models to function with imperfect data, flagging confidence levels based on completeness
The “Black Box” Problem and Clinical Trust
Many AI algorithms, particularly deep learning models, function as “black boxes”—they produce accurate predictions but can’t fully explain why. This creates tension in healthcare where clinicians need to understand reasoning to trust recommendations and maintain accountability for patient care decisions.
A care coordinator receives an alert: “Patient Smith has 87% predicted readmission risk.” If she can’t understand why—what specific factors drove that score—she may dismiss it as computer error or struggle to know how to intervene effectively.
Building clinical trust requires:
- Explainability: Use Einstein Prediction Builder’s feature importance rankings to show which factors most influenced each prediction
- Transparency: Clearly communicate model limitations, accuracy rates, and error possibilities
- Clinical validation: Involve physicians and nurses in model development and validation, not just IT staff
- Override capability: Enable clinicians to override AI recommendations with documented reasoning when clinical judgment differs
- Feedback loops: Show clinicians how their interventions based on AI predictions actually impacted outcomes
Alert Fatigue and Integration Friction
Healthcare workers already face overwhelming alert volumes from EHRs, clinical decision support systems, and communication platforms. Poorly implemented AI can exacerbate alert fatigue, leading users to ignore all alerts—including critical ones.
Similarly, if using AI-powered insights requires logging into a separate system, navigating complex interfaces, or disrupting established workflows, adoption will fail regardless of technical sophistication.
Design principles to avoid these pitfalls:
- Prioritize ruthlessly: Only alert on actionable insights requiring timely intervention, not interesting observations
- Deliver alerts in workflow: Surface Einstein insights within existing systems where work happens (EHR, care coordinator workspace)
- Enable bulk actions: Allow care teams to efficiently manage multiple patients (e.g., send education materials to all high-risk diabetics with HbA1c >9%)
- Optimize timing: Don’t interrupt clinical encounters; queue non-urgent insights for batch review during dedicated times
- Provide value quickly: Ensure the system saves time overall rather than adding work
Algorithmic Bias and Health Equity Concerns
AI models trained on biased historical data perpetuate and potentially amplify those biases. Healthcare has well-documented disparities in care access and quality across racial, ethnic, socioeconomic, and geographic lines. AI trained on this data can systematically underestimate risk or deprioritize care for already-disadvantaged populations.
A widely-publicized 2019 study found a healthcare risk prediction algorithm used by major health systems was significantly less likely to identify Black patients for care management programs compared to equally-sick white patients. The algorithm used healthcare spending as a proxy for health needs, but Black patients had lower spending due to reduced care access—not lower health needs.
Addressing bias requires:
- Diverse training data: Ensure model development includes representative populations across demographic groups
- Bias testing: Explicitly analyze model performance across race, ethnicity, language, socioeconomic status, and geography
- Outcome equity monitoring: Track whether AI-guided interventions produce equitable outcomes or widen disparities
- Regular auditing: Periodically reassess models for bias as populations and care patterns evolve
- Multidisciplinary oversight: Include ethicists, community representatives, and equity experts in AI governance—not just data scientists
Regulatory and Compliance Complexity
Healthcare AI navigates a complex regulatory landscape:
HIPAA compliance: AI systems must maintain appropriate privacy and security safeguards for protected health information. Questions arise around:
- Whether AI-generated predictions constitute part of the medical record
- How to manage consent for AI-based decision support
- De-identification requirements for model training data
FDA oversight: Depending on implementation, some AI tools may qualify as medical devices requiring FDA clearance. Generally, clinical decision support suggesting actions for clinicians to consider falls outside FDA regulation, while tools autonomously making diagnostic or treatment decisions may require approval.
Liability questions: If an AI algorithm recommends an intervention that harms a patient, who bears liability? The healthcare organization? The software vendor? The clinician who followed the recommendation?
Documentation requirements: Healthcare organizations must maintain clear records of:
- How AI models were developed and validated
- What data they use and how it’s protected
- Model performance metrics and limitations
- Clinical governance and oversight processes
The Resource Investment Reality
Successful AI implementation requires substantial investment beyond software licensing:
Technical infrastructure:
- Data integration and interoperability platforms
- Sufficient data storage and processing capability
- Ongoing Salesforce administration and development expertise
Organizational change management:
- Clinical workflow redesign
- Comprehensive training programs
- Ongoing support and optimization resources
- Leadership time to drive adoption
Data quality improvement:
- Cleaning and standardizing existing data
- Implementing standardized collection processes
- Ongoing data stewardship
Many organizations underestimate these requirements, focusing only on technology costs while neglecting the operational investments necessary for success.
Future Trends: The Evolution of AI in Healthcare
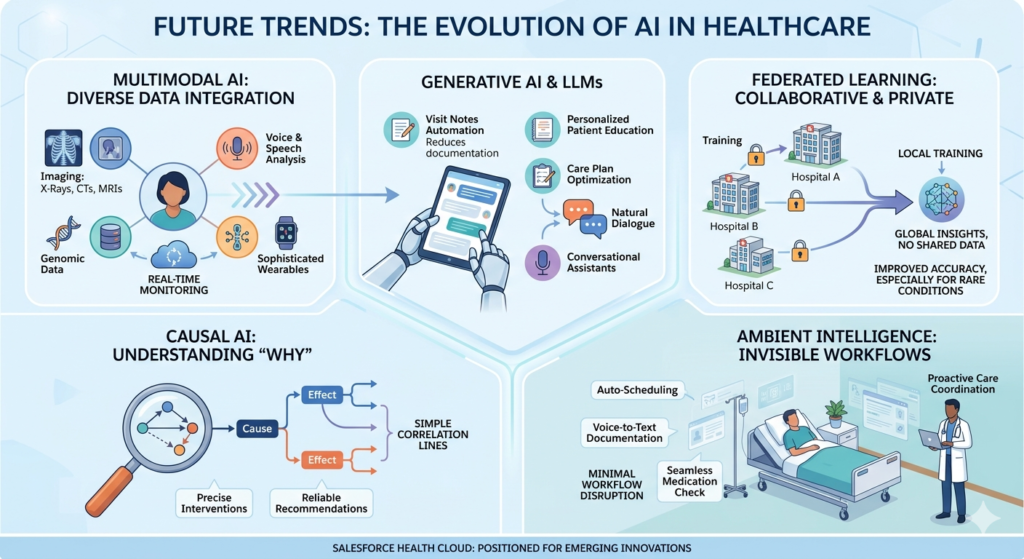
Multimodal AI: Integrating Diverse Data Types
Current healthcare AI predominantly analyzes structured data (diagnoses, lab values, vital signs) and text. The next frontier integrates diverse data types:
Medical imaging analysis: AI interpreting X-rays, CT scans, MRIs, and pathology slides could integrate with Health Cloud risk models. A patient’s lung cancer screening CT showing suspicious nodule automatically updates their risk profile, triggering care coordination workflows.
Voice and speech analysis: Research demonstrates that voice characteristics can indicate depression, Parkinson’s disease progression, heart failure exacerbations, and cognitive decline. Einstein could eventually analyze patient phone calls or voice messages for early warning signs.
Genomic data integration: As genetic testing becomes routine, AI models will incorporate genomic risk factors for disease predisposition and medication response, enabling truly personalized care plans.
Wearable device sophistication: Beyond basic activity and heart rate tracking, emerging wearables detect falls, monitor blood pressure continuously, analyze sleep architecture, and estimate blood glucose non-invasively. This continuous physiological data stream will enable real-time health status monitoring and intervention.
Salesforce Health Cloud’s extensible architecture positions it well to integrate these emerging data types as they mature clinically.
Generative AI and Large Language Models in Healthcare
The explosion of generative AI capabilities (ChatGPT, GPT-4, Med-PaLM) creates transformative possibilities:
Clinical documentation automation: AI that listens to patient encounters and automatically generates visit notes, extracts diagnosis codes, and updates care plans—reducing physician documentation burden by 60-80%.
Intelligent patient education: Rather than generic education materials, AI generates personalized explanations tailored to individual patient’s health literacy, language, cultural context, and specific clinical situation.
Care plan optimization: AI analyzes thousands of evidence-based guidelines, clinical trials, and similar patient outcomes to recommend optimized, personalized care plans that individual clinicians couldn’t manually synthesize.
Conversational health assistants: Beyond scripted chatbots, truly conversational AI that can discuss symptoms, medication side effects, and care questions in natural dialogue, appropriately escalating complex issues to human clinicians.
Salesforce Einstein GPT and integration with large language models will likely bring these capabilities to Health Cloud in coming years, though clinical validation and regulatory considerations will determine adoption timelines.
Federated Learning: Collaborative AI Preserving Privacy
A persistent challenge in healthcare AI is balancing data volume needs (more data creates better models) with privacy imperatives (can’t share patient data broadly). Federated learning offers a solution: AI models train across multiple healthcare organizations’ data without the data ever leaving its source.
Imagine 50 health systems collaboratively training a readmission prediction model. Rather than pooling patient data centrally (violating privacy and raising competitive concerns), each organization’s AI model trains on its local data, then shares only model insights—not patient information—to create a collective model benefiting from 50x more learning examples.
This approach could dramatically improve AI accuracy, especially for rare conditions where individual organizations have insufficient patient volume for robust model training.
Causal AI: Moving Beyond Correlation to Understanding
Current AI excels at identifying correlations (patients with characteristic X are 3x more likely to experience outcome Y) but struggles with causation (does X actually cause Y, or are both caused by unmeasured factor Z?).
Causal AI explicitly models cause-and-effect relationships, answering questions like:
- “If we implement this intervention, will this patient’s outcome actually improve, or are we seeing correlation without causation?”
- “Why did this particular patient respond to treatment while similar patients didn’t?”
This advancement will make AI recommendations more reliable and enable more precise, individualized care strategies.
Ambient Intelligence: Invisible AI Integration
The future of healthcare AI isn’t flashy dashboards and explicit recommendations—it’s seamless intelligence woven invisibly into all workflows:
- Scheduling systems automatically optimize appointment timing, duration, and modality based on patient needs without staff intervention
- Documentation systems capture clinical information automatically without physician typing
- Medication reconciliation happens seamlessly across care transitions without manual phone calls
- Care gaps close proactively without requiring coordinators to review reports and make calls
This “ambient intelligence” approach maximizes AI value while minimizing workflow disruption and cognitive burden on already-overwhelmed healthcare workers.
Regulatory Evolution: Standardized AI Governance Frameworks
As healthcare AI proliferation continues, regulatory frameworks will likely evolve from current ambiguity toward standardized governance approaches:
- Clear FDA pathways for different AI use cases
- Standardized bias and equity testing requirements
- Transparent algorithm disclosure expectations
- Liability frameworks for AI-involved care
- Accreditation standards for AI implementation quality
Organizations implementing AI now should anticipate this regulatory evolution and build governance structures that will adapt to emerging requirements.
Conclusion: The Strategic Imperative of AI-Powered Predictive Care
The healthcare industry faces an existential challenge: delivering increasingly complex care to aging populations with growing chronic disease burden while controlling unsustainable cost escalation. Traditional approaches—hiring more staff, working longer hours, incrementally optimizing processes—cannot bridge this gap.
AI in Salesforce Health Cloud represents a fundamental capability shift: moving from resource-limited reactive care to scalable, proactive, personalized care delivery. The organizations that successfully implement predictive care models will deliver demonstrably better patient outcomes while improving financial sustainability and clinician satisfaction.
The business case is compelling:
A typical mid-sized health system implementing comprehensive AI-powered predictive care across the use cases described in this guide can reasonably expect:
- $15-25M annual financial impact from reduced readmissions, avoided complications, shared savings program performance, and operational efficiency
- 15-25% improvement in key quality metrics (chronic disease control, preventive screening rates, patient safety indicators)
- 30-40% care coordinator productivity improvement through intelligent prioritization and workflow optimization
- Significant patient experience improvements through proactive, personalized engagement
Beyond immediate ROI, strategic benefits include:
- Competitive differentiation in value-based care contracts requiring population health management capabilities
- Risk-bearing readiness for transitioning from fee-for-service to capitation and shared risk models
- Clinician satisfaction through reduced administrative burden and tools enabling practice-at-top-of-license
- Data-driven culture establishing foundation for continuous improvement and innovation
The path forward requires:
- Executive commitment: AI transformation isn’t an IT project—it’s a strategic organizational initiative requiring sustained leadership engagement and investment
- Clinical engagement: Technology deployed without clinical input and workflow integration fails; successful AI requires physicians and nurses as design partners, not end users to convince
- Data foundation: Invest in data quality, interoperability, and governance before or concurrent with AI implementation
- Start focused, scale systematically: Begin with one high-impact use case, prove value, learn lessons, then expand—resist attempting to transform everything simultaneously
- Commitment to equity: Proactively address bias and ensure AI improves care for all populations, especially those historically underserved
- Continuous learning: AI improves with feedback; establish rigorous outcome measurement and model refinement processes
Healthcare stands at an inflection point. Organizations that embrace AI-powered predictive care now will define the future of patient care delivery. Those that delay risk competitive obsolescence as value-based payment models reward outcomes and efficiency rather than volume.
Salesforce Health Cloud with Einstein AI provides the platform. The vision, commitment, and execution to realize its potential rests with healthcare leaders willing to fundamentally reimagine how care gets delivered.
The future of healthcare is predictive, personalized, and proactive. The future is already here—the question is how quickly your organization will embrace it.
About RizeX Labs
At RizeX Labs, we specialize in delivering industry-focused Salesforce solutions, including advanced implementations of Salesforce Health Cloud powered by AI.
Our expertise combines deep technical knowledge, healthcare domain understanding, and real-world implementation experience to help organizations leverage Salesforce Einstein for predictive patient care.
We help healthcare providers move from reactive treatment models to proactive, data-driven care using intelligent automation, predictive insights, and personalized patient engagement.
Internal Links:
- Salesforce Admin & Development Training
- Remote Patient Monitoring (RPM) in Salesforce Health Cloud: Transforming Connected Healthcare Delivery
- How to Use AI in Salesforce Health Cloud for Predictive Patient Care (Einstein + Real Use Cases)
- New Releases in Salesforce Health Cloud Spring ’26: What Healthcare Organizations Need to Know
- How to Customize Salesforce Health Cloud Using Lightning Web Components (LWC) for Healthcare Use Cases
- 30 Essential Questions About Salesforce Health Cloud Answered: Beginner to Advanced Guide
- Salesforce Sales Cloud vs Health Cloud: The Strategic CRM Decision That Defines Your Healthcare Business Trajectory
- Using Salesforce Health Cloud for Insurance & Claims Coordination: Beyond the Hospital Walls
External Links:
- Salesforce Official Website
- Salesforce Health Cloud Overview
- Salesforce Revenue Cloud Overview
- Salesforce AppExchange (CLM tools)
- Salesforce CPQ Documentation
Quick Summary
AI in healthcare is no longer optional—it’s a competitive necessity. By combining Salesforce Health Cloud with Salesforce Einstein, organizations can predict patient risks, personalize care plans, and improve outcomes. From hospital readmission prediction to care gap identification, AI-driven workflows enable providers to act before problems escalate—reducing costs and saving lives.

